I’ve read the anonymous Trust guidance. It’s not sinister in the way that it has been interpreted. It only looks that way if you don’t really know how a death certificate is completed. https://drive.google.com/file/d/1JLsJ_iM0cehRXF6f8KUu-FDDY4Pr37b5/view
This ONS guidance on how to complete a death certificate explains well how it should be done correctly.
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/877302/guidance-for-doctors-completing-medical-certificates-of-cause-of-death-covid-19.pdf
I read through the trust “guidance” earlier but can’t get the google drives link to work now so am relying on memory.
It’s subtle.
I’ve written a good few (hundred) death certificates so I think I have a handle on how they work.
It is also worth remembering that, for in hospital deaths, the job of writing the death certificate usually falls to one of the most junior members of the team who, by extension, are also the least experienced and most susceptible to pressure to report the deaths in a particular way.
By saying “put pneumonia in 1a” and “no requirement to put Covid in part 1” a lot of ward doctors will take that as a signal that they should not be putting Covid on the death certificate, allowing it to be mentiond “should the doctor wish” further applies subtle pressure to not do so.
While I suspect that this document was written with the intent to help junior doctors know what to put on the certificate there are definitely subtle pressures within the guidance to avoid putting Covid on the form.
Helping junior doctors to know how to fill in the form is, in itself, reasonable - my recollection is this is one of many aspects of medical life where training is strictly on the job - most juniors never see the form until one is slapped in front of them with the instruction to fill it in and it can be pretty daunting when the degree of responsibility needed starts to dawn on you.
Not posted graphs for a couple of days.
Some cosmetic tweaking and a new reference line on the UK data - at the present rate we are on track to halve official new cases in roughly 35 days.
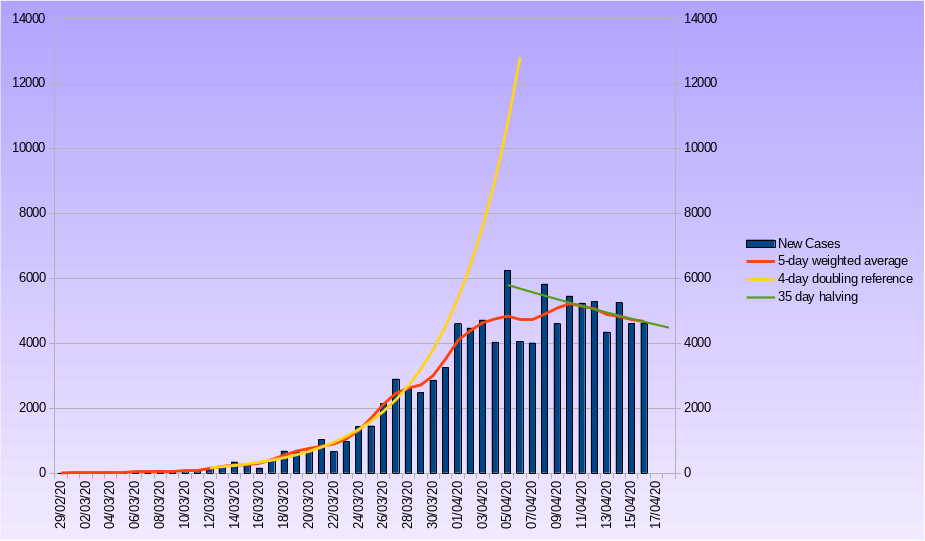
The problem with the UK numbers remain - no community data and, do you believe it anyway?
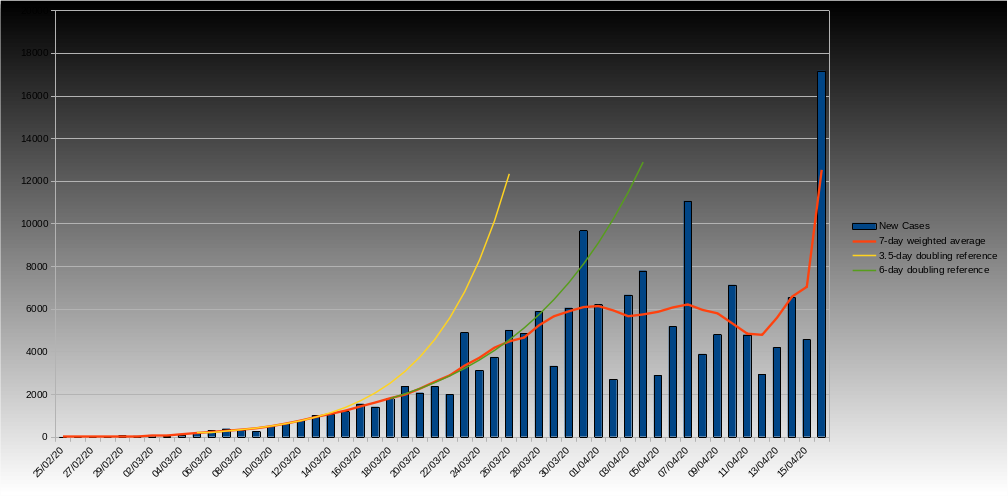
861 deaths were recorded today - lets assume that we are catching up on the reporting the lag over the Easter weekend.
French data - humm, anyone any pointers to where the massive spike comes from, have a chunk of delayed notifications from the community come in?
Just a thought (I am no clinician before I get shot down) but how are the CV care home deaths established?
There are not enough testing kits to test the staff, let alone all the residents so in view of the fact that no post mortem seems to be carried out the cause of death could well be random.
It may be difficult therefore to accurately determine the presence of the virus, let alone its role in the cause of death & this could skew the figures.
I also wonder how many of the non-hospital deaths are the result of those who should have sought hospital treatment for, say, a heart attack, a fever or some other illness not actually getting it because they do not want to add to the NHS workload/worried about contracting CV/not being considered to be an urgent case?
I am still not clear as to how many people who were fit & healthy have died solely from the virus rather than it being just a contributing factor, in which case would it not be difficult to determine the precise cause of death?
Finally, much as I am no fan of the UK’s current government, it does seem a little hard to blame them for nursing homes not having enough PPE. After all, most of them are privately run & charge handsomely so they should provide their own.
There was a big thing on the BBC the other day to encourage ill (none Covid ) patients to still attend A&E as numbers are dropping and some serious illnesses are being missed also people with early cancer symptoms aren’t presenting to their doctors
1 Like
I understand your point @anon90504988 but even whole Countries have had difficulty obtaining supplies when America First raided world supplies…
Coronavirus: A&E visits drop sharply as calls to 111 double https://www.bbc.co.uk/news/health-52232941
I tend to agree with you Mark. Having seen my father in a private ‘nursing home’ at the end of his life, there was one registered nurse who seemingly seemed to work about 18 hours a day surrounded by ‘carers’ who probably had minimal training and would not have had a clue about PPE in terms of protection from things like Coronavirus. I suspect the private sector have the same issue currently of obtaining enough / the correct type of PPE required. I have to say the care was amazing but at 6000 pounds per month it needed to be.
1 Like
Sympathetic to this PoV but PPE very hard to get hold of at the moment and efforts to do so probably should be co-ordinated centrally.
2 Likes
I’ve not written hundreds of death certificates as I work in Emergency Medicine & only ever get asked to write one every couple of months. We don’t actually have many patients die in ED as we are usually able resuscitate them sufficiently to get them to the ward. I wouldn’t be able to sign a death certificate for a number of those who die anyway as the cause of death is unclear. At one time we had to refer all deaths within 24 hours of hospital admission to the coroner but they relaxed this requirement a few years back.
I still think that the advice is quite neutral & the same advice would apply if the causative agent was influenza.
One unfortunate side effect of the climate of fear whipped up by the media & politicians (although this is maybe required to ensure people adhere to lockdown & social distancing) is that people wildly overestimate the risks of dying from COVID-19.
It’s not just the risks of dying though it’s being very ill,passing it to those you live with etc
1 Like
On a personal level?
Indeed though as a House Officer/SHO (or FY/CT doc as currently) one a week for the first few years of your career is not unreasonable and I think most doctors would run up 1-200 in that situation.
I worked on a stroke step-down ward for a year, quite a lot of patients transferred from the acute unit for EOL palliative care - I suspect that bumped up my tally quite a bit.
I don’t think anyone would write a document such as that and actually give incorrect advice - but there is a definite difference between encouragement to put Covid if it is a possibility and encouragement to avoid Covid on the form unless there is certainty - and I think it leans to the latter.
We know there is systematic under-reporting, however you read that advice regarding death certificates, because only in-patient deaths where there is a positive test result are bing recorded.
1 Like
Probably 50-60% of those with COVID-19 infections are completely asymptomatic. Another 35% have symptoms varying from a cough & sore throat to a flu like illness requiring bed rest & paracetamol. 10-15% have more severe symptoms & require hospital admission of those perhaps a fifth need ICU. If you get admitted to ICU there is a 50% chance you won’t survive.
Overall mortality might be 0.5-1%. I’m 66 & my average chance of dying in the next year is about 1% but that doesn’t keep me awake at night. If you are 80 then you have on average a 10% chance of dying in the next year but again I don’t think many 80 year olds worry too much about those odds.
In the UK
75% of those who die are male
75% of those who die have a BMI over 25
35% of those who die are non-white (might be over reported at present due to hot spots in London & West Midlands)
The way people assess risk of illness & death has an awfully of emotion attached which is people wildly overestimate the risks of dying from COVID-19.
Then you read stories like these (and there are many like them)
and you realise that it can happen to anyone.
Of course we have no idea if the stories that get into the press are exceptional or whether they’re the tip of the iceberg and there are thousands like it that go unreported. But it seems unlikely that the press gets hold of them all, or indeed that every family allows its grief to be made public.
1 Like
There are always sad cases of previously healthy people dying but the numbers as now are always very very low. These cases are exceptional & while they might previously have been reported in local media now it’s publicised nationally. Each month in both France & the UK around 50,000 people die that’s around 1700-1800 a day at this time of year. As I pointed out previously on average your chances of dying of COVID-19 are the same as dying of any cause in the next 12 months. Most people even nonagenarians don’t think twice about their chances of dying in the next year.
Broadly I’d agree with the figures you quote - I’d put a slightly different slant on it based on the UK data/experience which would be:
- up to 66% asymptomatic, no one knows and unless there is population based testing we won’t know.
- of symptomatic patients many are mild and most of even the more severe ones are not deemed ill enough to be sent to hospital by the 111 service; maybe 10% hospitalised
- if you are ill enough to be admitted and are not the Prime Minister you have about a 30% chance of dying
- if you are ill enough to get to ICU (and are not the Prime Minister), you have a 50-80% chance of dying.
Should be “In the UK ICUs”
The Spiegelhalter “paper” quoted 95% CI of 0.4-1.4% which seems to be about where most of the estimates fall at the moment - which is higher than the 0.1% IFR typically quoted for 'flu.
However I will reiterate - that 0.9% average fatality estimate is only bought with the present level of lockdown - if you let up and the number of cases swamps the NHS it will be much higher.
In fact I suspect that the overall UK fatality estimates will be at the upper end of global figures, given the initial, misguided “herd immunity” approach (which seems to be alive and well albeit in covert form).
It makes one hell of a difference if it is you are one of the people that needs hospitalisation.
My friend Lynn McBride, who used to live near Cluny and now in Beaune, is American and she and her husband went back to Charleston for some time in the winter. She flew to Washington for a three day reunion with friends and came back with symptoms of Covid.
You can read the harrowing diary she kept on her blog ‘Southern Fried French’. She narrowly escaped hospitalisation but, at one time was talking what her husband should do if she died.
No way do I want to have to repeat her ordeal.
I can’t think of many illnesses that kill you that quickly though.
Yes I might die of cancer within the next 12 months - but I would probably (not necessarily) be expecting it.
Ditto heart disease.
Ditto kidney failure.
In theory I follow your argument, but it practice it doesn’t ring quite true. Logic tells me that the odds were strongly against these healthy young people dying of cancer, heart disease or suchlike. If you limit yourself to looking at statistics, yes - they are people, and people die. But if you look at them as individuals then no, because they don’t fit the profile for cancer or heart disease deaths. There is no known profile for covid19 so everyone’s chances appear to be equal, be they old, young, obsese, fit - all the things that change the odds if you look at them as individuals.